Head Shape in Infants and Craniosynostosis
Concerns about head shapes in infant
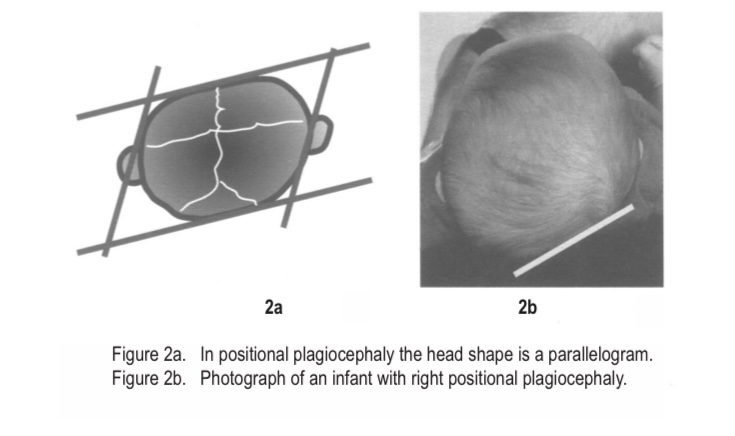
Concerns around abnormal head are not uncommon. The majority will have normal variants (such as positional plagiocephaly and benign metopic ridge) but it is important to assess for craniosynostosis by looking at the babies head from above and refer early if concerned
Differentiating Craniosynostosis from Normal Variants
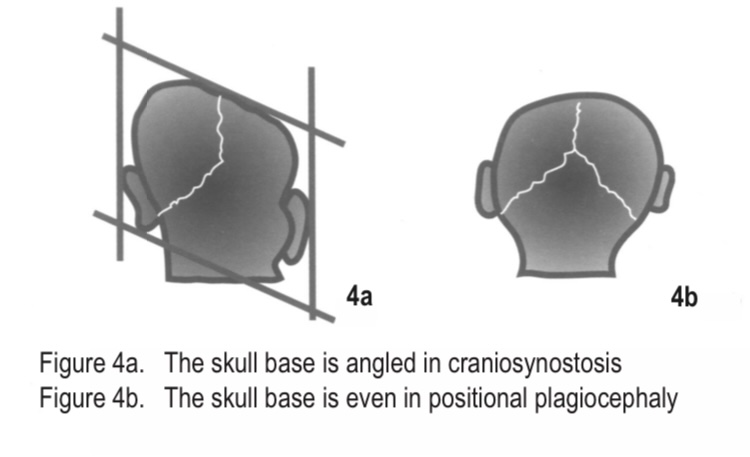
Look at the overall head shape from above and position of ears relative to each other. In positional plagiocephaly the ear and forehead on the ipsilateral side to the flattening will be anteriorly placed when viewed from the top. See figures below for assessment from top and back of head.
Top
Back
(Source: BC Children’s hospital guide)
Benign Metopic Ridge Metopic cranisynostosis
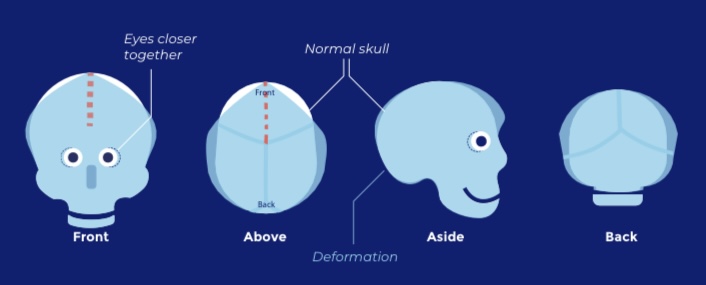
Metopic craniosynostosis differs from a simple metopic ridge by absence of forehead flattening, creating a triangular shape.
 (Source: European Reference Network Cranio)
(Source: European Reference Network Cranio)
Key Points on Clinical Assessment
History should include timing and progression of abnormal head shape, symptoms of raised intracranial pressure, antenatal, neonatal and family history
Physical examination should assess head shape (front, above and side), head circumference, anterior fontanelle, any ridges or bulges, and associated dysmorphic features or anomalies.
What to Do If Craniosynostosis is Suspected
Refer. If craniosynostosis is strongly suspected and no acute concerns consider also sending details and pictures to our specialist craniofacial unit - in our case Oxford Craniofacial Unit. Details on referral advice and guidance contacts available here Oxford Craniofacial Team
Why Time Matters
Early diagnosis and intervention - before 6 months of age ideally - is crucial to avoid limitations on surgical options as the child ages and skull bones become less malleable